Introduction
Awareness of obsessive compulsive disorder (OCD) in the United States has grown significantly over the past 10 years. The American public has even developed a kind of fascination with the condition as evidenced by the it’s presence in reality TV shows, film, and literature. OCDism has also made it’s way into popular culture and slang: “you are ocding… that is so OCD… I am obsessed”. This popularization of OCD, however, has been a double edged sword: on the one hand it has helped remove some of the stigma typically attached to psychiatric disorders; on the other, it has also trivialized the condition. While it is true that fleeting intrusions and minor compulsions are normal, OCD, the disorder, is far from a curious entertainment; rather it is a serious-and often chronic condition-that can lead to horrible suffering and even disability if not treated.
Definition Of OCD
The American Psychiatric Association diagnostic manual (DSM-5) defines OCD as a condition characterized by the presence of either obsessions and/or compulsions” that occupy at least an hour per day of the person’s time. Obsessions are characterized by recurrent and persistent thoughts and/or images that are experienced as intrusive, unwanted and disturbing to the extent that the person is driven to Compulsions, the response to obsessions, intended to undo or “neutralize” this distress. These include a wide range of repetitive behaviors and/or mental acts such as checking, washing/sanitizing, counting, repeating, thought suppression.
Compulsions or neutralizations can range from simple behaviors to very complex rituals that must rigidly conform to idiosyncratic multistep rules. Neutralizations can also be ”overt”, visible behaviors or "covert", such as mental reviewing, rumination, reassurance seeking or avoidance. As noted above, individuals with OCD neutralize to diminish the distress obsessions create; but this relief is short-lived, as the obsession soon recurs, and the cycle is repeated, which only further increases anxiety and depletion. The complexity of this recursive cycle will be further explored elsewhere on this page.
Most individuals with OCD recognize that their obsessions are not reasonable. However, there is a broad continuum of such insight in OCD sufferers. For those with poor insight, the line between real and imagined becomes blurred. This should not be confused with the momentary loss of rational thinking, while acutely anxious, that even sufferers with good insight experience when faced with an obsessional trigger. Those with poor insight are not able to see the line between imagination and reality, even when they are far removed from their OCD trigger situations. However, individuals with even moderate insight, are able to see the irrational nature of their obsessional fears between challenges. As a result, those with low insight are less likely to engage in treatment and, when they do, are more resistant to treatment interventions.
Subtypes and Dimensions of OCD
In the 1930s, psychologists began to divide OCD by subtypes based on compulsions, such as washing, checking, repetition, etc. In the 1970s, researchers started to develop questionnaires to identify subtypes of OCD based on symptoms. In the past 15 years, most psychologists, who study OCD, have argued that newer measurements suggest that beyond subtypes there are dimensions of OCD that can be grouped together based on themes and/or symptoms. While the addition of a dimensional perspective better captures the diverse and complex nature of OCD, researchers disagree about the dimensions themselves, whether they should be grouped by theme or by symptom and whether subtypes should be used along side dimensions.
The scientific categorization of OCD has no doubt advanced over the past 80 years. Yet a unified system that captures the diagnostic complexity, etiology and best practices is still a work in progress. Another possibility is that as the science of genetics and neuroscience advances, the broad net of what we call obsessive compulsive disorder today will eventually be identified to be distinct syndromes with overlapping features. Moreover, while I believe it is important to have a general understanding of the evolution of diagnostic categorization, I feel that in clinical work a broad brush better lends itself to the practical tasks of identifying, understanding and treating OCD as we know it. To that end, I have organized the following abbreviated descriptions of the most common categories of dimensions (or subtypes) I see and treat in my practice.
CONTAMINATION-WASHING
Fear of contamination by bacteria, viruses, chemicals, environmental pollutants or by thoughts or acts that one finds disgusting or morally reprehensible. Compulsive responses involve,repeated washing, cleaning and sanitizing. It is important to emphasize that in contamination OCD there is as much or more avoidance as there is sanitizing. There is also the concept of chains of contamination: “ He touched, the doorknob and is sitting on the couch. I will be contaminated if I sit on the couch”
DOUBTING-CHECKING
This is the almost iconic “checking compulsion”. Obsessions involve fear of an oversight concerning locking, turning off of doors, windows, stoves, lights, faucets, cars or having hit someone while driving, but can include anything where there is potential of harm to oneself or others. Doubting obsessions can also theme of perfectionism involving fear of mistakes, fear of not doing something well enough and underlying fear of being an imposter, known as Imposter Syndrome
There follows repetitive, incessant, and sometimes very prolonged, checking of these objects or actions as well as checking of writing, assignments or work, which only reinforces the illusion that something has been overlooked. The role of distrust of perception along with distrust of self, in this checking subtype, will be subsequently explored as this page is developed.
FEAR OF MISTAKES-PERFECTIONISM DOUBTING AND CHECKING OCD
Obsessions of having made a mistake and not having met self-imposed, extremely high, “perfectionistic “ standards in some type of endeavor, task, action. This can be triggered by any situations where there are perceived performance-related consequences, but typically involves work, school or personal commitments. The compulsive responses to this obsession are endless: checking and reviewing of what has been done, scouring for any mistakes or errors that might have been made. The fear that something could have been missed or that the work done is simply not good enough only drives further checking and reviewing. As with harm-based doubting such repetitive checking brings no resolution. In fact, the frantic scan and hunt for the mistake leads to increased doubt, self distrust and confusion.
Tormenting Obsessions-Unwanted/Unacceptable Thoughts
This subtype is characterized by the experiencing of thoughts, intrusions and/or images that are unwanted and considered unacceptable, repugnant and/or immoral- that run contrary to the person’s values or ethics. Themes are unique to the person, but commonly involve violent, sexual, racist, religious content and can include sexual identity, sometimes referred to as “homosexual OCD” (H-OCD). With regard to the latter, I have also seen the reverse: a lesbian fearing that she was straight. So, again, the uniqueness to the person factor is important.
In the past, this subtype has been referred to as “Pure O”, under the assumption that there was not a corresponding “compulsion”. This is no longer the prevailing view, as indeed there is always some form of (neutralization) response to the obsession, but it is also mental in nature. For example, a person might experience the obsessional doubt “what if I stabbed by spouse”, which is followed by the mental neutralization of visualizing throwing away the knife or mentally repeating reassuring statements, such as “ I would never do that “. Yes, both are purely mental in nature. However, while the first is the the intrusive obsession and second is the response ( compulsion or neutralization). But there is no pure obsession. In fact, the compulsions in this subtype are rarely just mental but involve many types of behaviors: distraction, complex avoidance, praying, confessing, reassurance seeking, etc. An example of tormenting obsessions in the postpartum can be found on the Maternal Anxiety page
Symmetry, Ordering, Precision, Just Right Counting
Onset of this subtype is typically seen in childhood and is characterized by the need for precision, exactness, completion, exactness or “just rightness”- that some researchers refer to as “sensorily-based perfectionism". Compulsions are directed toward achieving this state of just-rightness. Examples of these typically include arbitrary rules of ordering, arranging objects by categories, positioning, straightening to achieve evenness, symmetry or left-right balance. Compulsions involve, but are not limited to, turning devices or fixtures on and off such as lights, electronics, appliances, faucets. There can also be repetition behaviors-that can be ritualized or not- such as tapping, touching, stepping-or not stepping-on certain things, cracks, sidewalks, etc.
Almost universally, those with this subtype report a physical, urge-like “need” to complete the compulsion and the experience of intense, physical tension when attempting to resist these compulsions. For some, this tension can become almost unbearable, resembling, at times, the build up of tension experienced in tic disorders. Not surprisingly, it appears that co-morbid (co-existing) tic disorders are more prevalent in this subtype.These obsessions often-but not always-can be accompanied by magical or superstitious beliefs that something “bad could happen”-usually to a loved one-if the compulsion is not acted on. For the sake of simplicity, in this grouping, I have included counting, which some might argue could be categorized separately. However, with counting compulsions, many of the completion, symmetry and/or rule-driven characteristics described above also occur. Counting often goes beyond numbers and repetitions, but often includes, angles, spaces, relationships between numbers, etc.
Treatment
Three models of treatment will be discussed in this section:
- Exposure and Response Prevention (ERP) and Cognitive and Behavioral (CBT)
- The Cognitive Model (CT)
- The Inferential Based Approach ( IBT)
Behavioral Therapy
Behavioral therapy for OCD is the predominant treatment approach in the US. The primary intervention, Exposure and Ritual Prevention (EX-RP or ERP), first developed by Meyer in the 1960s, involves prolonged exposure to situations that cause distress or fear combined with prevention of “ritual completion”. An example would be repeatedly touching a doorknob and resisting urges to wash until contamination obsessions fade. ERP is the most researched approach and consequently, there is a significant body of evidence supporting it’s effectiveness. At the same time, a well documented problem with BT/ERP is that many cannot tolerate the distress the treatment causes. Consequently, roughly 40% of those treated with ERP either don’t complete exposure tasks or dropout.
To address this limitation, behavioral therapists began to use some cognitive therapy techniques-such as cognitive reframing (looking at the evidence for and against a particular fear)-prior to the ERP phase of treatment. Although research demonstrated some decrease in both drop-out and relapse, the ERP component was not modified and, as with ERP alone, remained difficult to tolerate.
I briefly treated OCD with ERP-based CBT, but found that there were aspects of ERP that seemed unnatural and unnecessary. While it made sense that someone with contamination obsessions tolerate the distress of touching a doorknob; it did not make sense- or seem appropriate- to have someone lick her fingers after touching a toilet seat or purposely make a mistake on a paper for school. That goes beyond the bounds of reasonable or rational. I also found that the cognitive techniques used by proponents of this hybrid approach, were mere window dressing within the ERP model.
There is a narrative in certain segments of the American OCD treatment community that ERP is the only effective evidenced- based method to treat OCD. This is simply not true.
ERP is particularly problematic, in my opinion, when used to treat tormenting obsessions. ERP for obsessions uses a technique called “imaginal exposure”, which involves first scripting out the obsession to it’s catastrophic and horrific end and then listening to this on a looped tape repeatedly . For example, someone with obsessional fears of harming his/her child, would write out the specific act of harm, in detail, from start to finish, including all the consequences that would follow, including loss of family, a life of isolation, incarceration and despair The person would then repeatedly listen to this horrific scripted narrative on a looped tape or mp3 until they are numbed to the obsession and thus "desensitized".
While some are able to tolerate imaginal exposure and desensitize, others can not. In fact, for those more vulnerable individuals, repeatedly listening to these scripts of horror, can be so unbearable that they stop therapy. Those who do drop out, however, can find themselves stuck in an ERP nightmare, clinging to the hope that they are “ just having obsessions”, yet terrified that the horrific content of these could be a sign of mental illness and consequently acted on. Left in this form of treatment limbo, they can sometimes resign themselves to “getting by” and “living” with their OCD; or, if more resourceful, they continue to look for other treatment options
There is a narrative in of the American OCD clinical community that ERP is the only evidenced-based method that is effective in the treatment of this disorder. This is simply not true. Yes, ERP, having been around since the 1960s, has accumulated the most efficacy research; but over the past 20 years, there has been a growing body of research demonstrating the efficacy of cognitive therapies that use other techniques and tools. I have seen many “ERP refugees”, who achieved success in overcoming their tormenting obsessions in ways they did not doing ERP. As this page is developed, I will further elaborate on my disagreements with this and other aspects of ERP. But for now, let if suffice to say that these early experiences cemented my belief that when treating OCD, understanding and addressing the complex cognitive processes at work is essential.
Cognitive Therapy (CT)
The cognitive model of OCD was first introduced in the 1970s, adapted Aaron Beck’s cognitive therapy to the treatment of OCD. In this model, “intrusive thoughts are [considered] normal phenomena experienced universally by people with and without OCD”. People without OCD simply dismiss these intrusive thoughts as meaningless and ignore them; whereas those with OCD go on to interpret intrusions through the lens of their “maladaptive beliefs”, such as exaggerated responsibility, intolerance of uncertainty. These appraisals cause distress and/or fear driving the person to “neutralize the obsession”. But relief is short-lived, and the simply cycle repeats itself.
Treatment in the cognitive model involves challenging these interpretations. Through socratic questioning of the evidence for and against such interpretations, the client is guided to develop an alternative “hypothesis”- another way of viewing the intrusion. Instead of exposure, per se, cognitive therapy uses behavioral experiments- to test the alternative “hypotheses” developed through cognitive reframing. Behavior experiments by definition also involve not acting on the compulsion (or ritual prevention, in the language of BT). In CT a situational triggers are gathered and organized into hierarchy of difficulty. Progress, in behaviorally measurable terms, is also monitored.
For a checker this could be leaving the house without checking the stove, thus, reinforcing perception of reality: “ I really can trust what I do.. I can trust my memory… I am a responsible person, my fears are is farfetched”. In the end, there has been no fire or break-in; but this was achieved without checking, which undermines the narrative that compulsive checking is necessary to avoid disaster.
With regard to tormenting intrusions, the cognitive model views these as a benign “firing off” of the mind that occurs commonly in the general population. When given meaning, however, according to this model, one goes on to develop obsessions. Treatment interventions, however, for tormenting obsessions do not involve looped tape exposure and desensitization as in behavioral therapy. Rather, the focus is on challenging the erroneous interpretation of intrusions while facing situations avoided and dropping safety behaviors such as reassurance seeking or mental reviewing. Over time, the person is able to see that there obsessional fears were unfounded, and ultimately the person is able to regain trust in themselves and recover normalcy. Again, because neutralizations were resisted, the corrective outcome cannot be attributed to "protective" measures that were taken.
I shifted to the cognitive model of OCD and went on to train in cognitive therapy for OCD with Gail Steketee, a clinical researcher, who-together with Sabine Wilhelm, had just developed a new treatment manual based on cognitive methods. I immediately found the approach to be far more rational, relevant and effective than ERP alone. The contribution of the cognitive model of OCD can not be understated. By looking into how mental processes work in OCD, individuals gain insight that is paid forward when tolerating distress during the challenging tasks of behavioral change that must be tackled in treatment. In my experience, cognitive therapy offers the benefits of insight, rational behavior change goals and consequently improved results and decreased drop out
Unfortunately, as much of a step forward that cognitive therapy represents, there are, in my opinion certain limits of the model in the treatment of OCD. Cognitive therapy was developed in context of treating depression. People with depression can let beliefs of negative outcome, for example color their appraisal of certain situations. These biased interpretation of events negatively affects mood and, in turn, behavior. In therapy, such “automatic [distorted] thought(s)” are identified and corrected; new behaviors are initiated in line with the corrected view, and there is change. This is tried and true, and, in my experience, theory lines up with clinical practice
This model, however, does not flow in the same way when applied to the very different cognitive processes and interpretive sequences that characterize OCD. Seeking to maintain the causal role of distorted interpretations, the cognitive model attempts to fit a (depressive) circle into a (obsessional) square. In order to accomplish this, the phenomenon of intrusions is dismissed as a simple hiccup of the mind. Hence, the cognitive model posits that “intrusions” are common to "everyone" and not specific to OCD; and it is the maladaptive interpretation of these that leads to obsessions. According to this model, challenge the interpretations of the intrusions that “everyone has”, test new behaviors, and you achieve change.
But is true that OCD starts with the interpretation of intrusions that “everyone has”? Someone with contamination/washing OCD will fear they might be infected with HIV after touching a box in the supermarket also contaminated with HIV. But does "everyone" have the intrusion that HIV is everywhere in the supermarket, waiting for a hand to touch it ? Is it the interpretation of this "common" intrusion that distinguishes those who go on to have OCD and those who do not ? Or, are there cognitive processes operating at a more granular level not captured by in this model ?
The Inferential-Based Approach (IBA)
The Inferential Based Approach (IBA) was developed in the late 1990s by Kieron O’Connor, a clinical researcher at the University of Montreal. In contrast to previous cognitive models, obsessions, in IBA, are not the product of "maladaptive" interpretations of intrusions. Rather obsessions are constructions of doubt that emerge from a disordered form of reasoning. In "normal" reasoning, we infer probability from real circumstances about which there is direct evidence. We can also experience "normal" doubt about real situations that have uncertain outcomes. But normal doubt can be resolved from the same source of reality from which it was born.
In a doubting inference, imagination and/or implausibility override and replace trust in perception and direct evidence
For example a dad sees his son sitting next to a cookie jar, and wonders if he has taken a cookie. He then observes cookie crumbs on the floor and chocolate around his son's mouth. It is reasonable for this dad infer that his son got into the cookie jar. The son, cookies, crumbs and chocolate all exist in the relevant context of what is known about cookie, kids and his son.
In obsessions, the rules of normal reasoning do not operate, as a narrative of doubt is inferred not from perception but from "a hypothetical premise" involving a feared outcome that is imagined or implausible. This upside down type of thinking gives rise to "inferential confusion", where imagination and remote (irrelevant ) possibilities are treated as real and plausible. These constructed, imagined stories cascade "downstream" into an abyss of often horrible albeit imagined consequences laden with powerful negative emotions that override trust in perception and overwhelm efforts to recapture rational thinking. A call to compulsive action ensues in an effort to neutralize the obsessional threat. However, this defensive response to what is merely an illusion only breaths more life into the obsession. In this way, the obsessional process completes its journey from mental construction to lived-in experience.
To illustrate this process, let's return to the example of fearing contamination by HIV in the supermarket. A person with OCD generates an imagined story that defies all known science as well as what their senses perceive and projects the idea, or illusion, that HIV could somehow be on a box in a supermarket. Confusing the imagined scenario with reality, the person infers threat of contamination, and avoids the touching the box. By neutralizing in this way and treating the constructed story "as if" it were real, the obsession becomes "lived in".
At this point, the person follows the internal logic of the obsessional narrative and goes further "downstream" in the story by imagining the meaning or consequences of having HIV. This leads to an intense emotional immersion in the obsessional doubt, which inevitably further distances the person from the starting point or cross over from reality to obsession. It should be noted, however, that the depleted mood that results from imagining "having HIV", in OCD, is very different than the distorted interpretations of real situations that are observed in primary depression.
Another example of this process can be seen in the doubting-checking sequence illustrated below:
- You close and lock a door and see that it is closed and locked.
- But you distrust what your eyes see, and you think that perhaps the door is really open.
- You think about a possible consequence of being robbed
- Because you think about the consequence you experience fear and distress.
- You then go on to check the door.
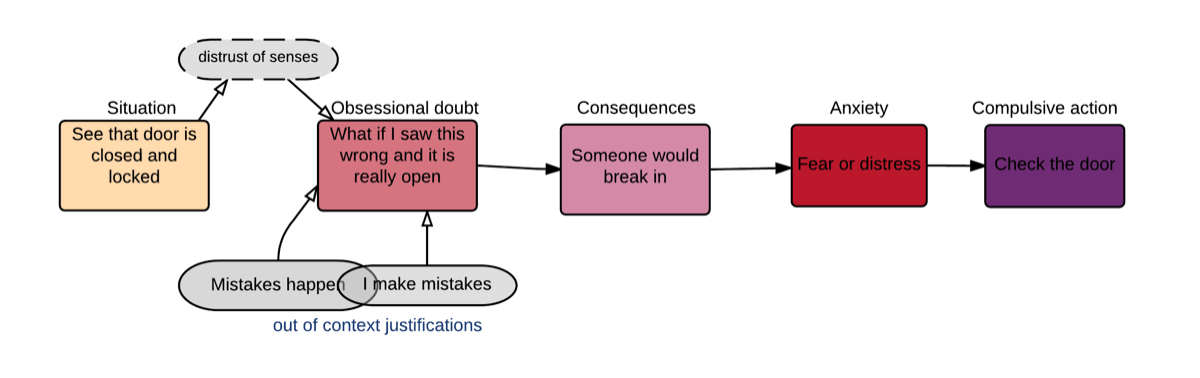
Again, illustrated in the sequence above, OCD starts by “crossing over” from reality to imagination (or the extremely implausible). In this cross-over, there is a confusion between what really is and what could be. In this sequence, there is an inference drawn from the possibility that the door could be unlocked, in spite of evidence to the contrary. That doubting inference-that the door could be unlocked-becomes lived in when one actually checks the door (compulsive action or neutralization). Acting on the urge to check gives quick relief but reinforces the unfounded fear that the obsessional doubt could be real.
Below is a more elaborated graphic model of doubting and checking that includes the process of "crossing over" from perception to imagination, the ensuing inferential confusion, the impact on emotion, the downstream secondary inferences and interpretation which lead to compulsion or neutralization. This model also shows the dynamic interplay between components of the process, which ultimately is self-reinforcing
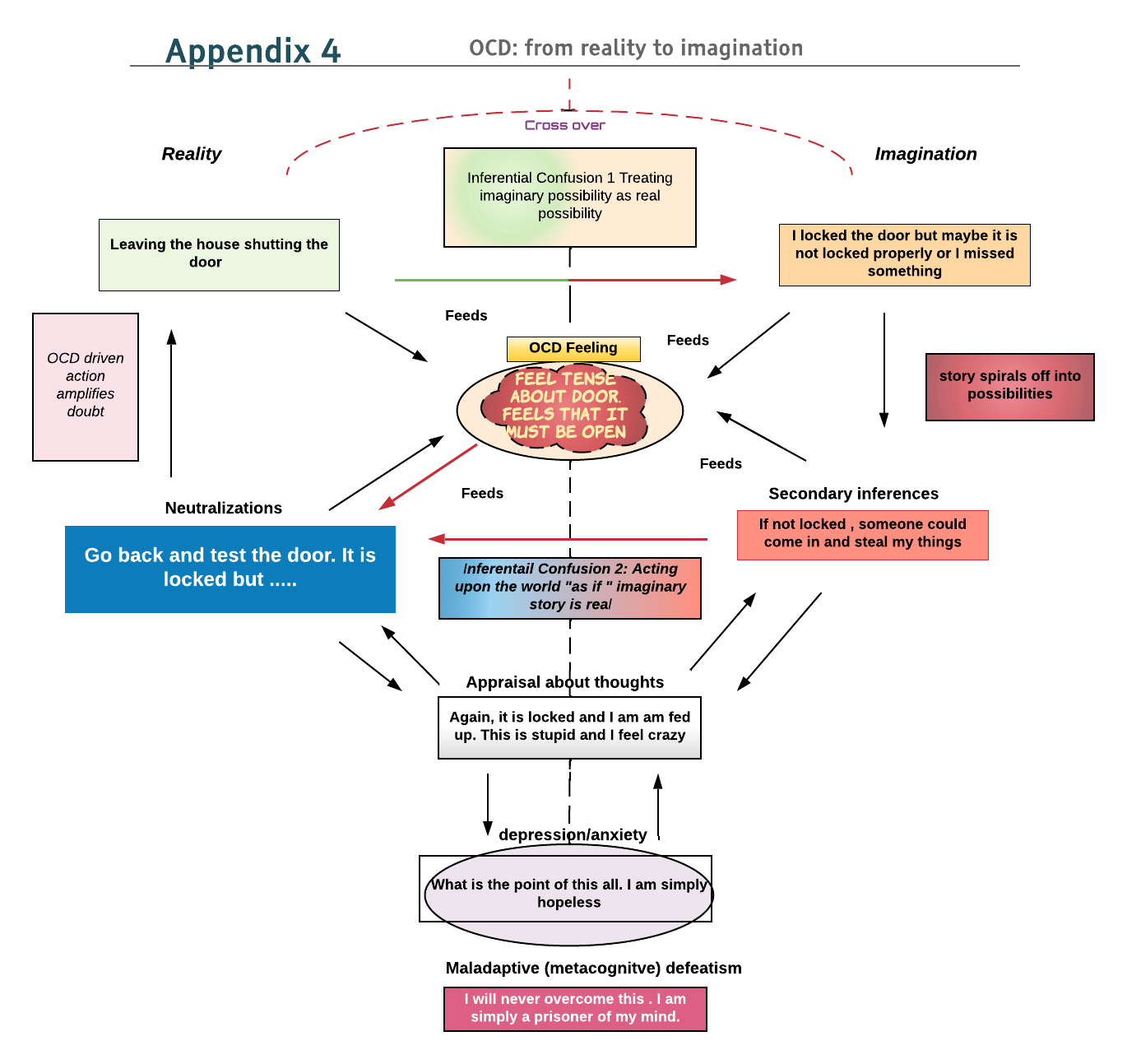
Obsessional doubt is born of imagination and internally projected possibility scenarios that are 100% irrelevant to the here and now.
This model illustrates what anyone with OCD knows: compulsive action is not a way out, but a fast train back to the obsession. In fact, there can never be a resolution to obsessional doubt, as you can not resolve something that doesn’t exist to begin with. This is simply chasing shadows which seeds the next round of doubt
Inferential-Based Treatment (IBT)
IBT-starts with a multi-dimensional assessment that combines questionnaires and interviewing to identify the specific sub-type(s) of OCD in question. Co-existing anxiety disorders are also identified during this process. IBT is a structured program divided into 3 parts. Each part, in turn, is organized into a series of steps. While there is a developmental progression through these phases of treatment, goals often are fluid, as therapists often adapt the program based on the subtype in question, client's self narrative and unique learning style, inform the way the IBT model is presented
The IBT Program Structure
| The steps Covered | Part One: Education | Part Two: Intervention | Part Three: Consolidation |
|---|---|---|---|
| Step 1 | When doubt begins | OCD is 100% Imaginary | A different Story |
| Step 2 | The Logic Behind OCD | Doubt and Possibility | Tricks and Treats of the OCD Salesman |
| Step 3 | The obsessional Story | The OCD bubble | The Real Self |
| Step 4 | The vulnerable Self | Reality Sensing | Out into the World |
IBT Summary Points
- Obsessional doubt is the starting point for OCD and it 100% imaginary and always originates from within the person
- There is direct evidence for normal doubt and therefore it has a resolution. (Will it be a long winter). Obsessional doubt is born of imagination and internally projected possibility scenarios that are 100% irrelevant to the here and now. Consequently, there can be no (here-and-now ) resolution to obsessional doubt (You can imagine that a closed door might not be closed, but checking what you have imagined brings no resolution; it merely reinforces doubt and imagination.
- In OCD doubting there is a selective and arbitrary relationship with possibility. A .01% chance of a feared event occurring is not enough reassurance. Rather the person wants 100% and/or a certificate from God. Yet, the possibility rules change for this event; and the certificate is no longer needed.
- Because OCD is 100% imaginary, there is a distrust of the senses, common sense, relevant evidence.
- In OCD there is a “cross over” from the real to an imagined OCD bubble. It is important to discover these cross over points ( remember the door example above)
- Because sequences in the obsessional chain of thinking do not have a basis in the here and now, there is never linkage between these sequences in reality. They are instead justified by references to other contexts, events, actions or by arbitrarily invented rules. (People make mistakes, so maybe the door was locked and I didn’t see it)
- Change in IBT begins with taking apart and unmasking the illusion behind the obsessional story. An alternative narrative is then built based on trust in the senses, common sense and perception This alternative narrative leads “to an entirely different conclusion than that of the obsessional doubt”. [My mind has tricked me into not believing that the door is not locked by pointing me toward thinking about doors elsewhere that are unlocked. However those doors are not my door. My eyes work fine and they see that my door is locked and will trust what my sense tell me]
- In IBT, changing behavior involves the testing of a rediscovered trust in reality, and is termed “reality sensing”.This step into action highlights that obsessional doubt is always false “because it goes against reality. Reality sensing is “simply trusting and going with the senses rather than doubting and going away from them”.
- Reality sensing, thus, takes the lived-in obsessional "prison" and turns it on it's head by traveling down a path grounded in what is. The counter-obsessional narrative, thus, becomes lived in. [I know that the door is really locked because my senses see this. Not checking a door that is seen to be locked reinforces the commitment to the world as is.
- A phase in IBT involves identifying "The Vulnerable-Self Theme" that is present in all of us but significantly more so in people with OCD. The vulnerable self theme "locates the OCD within a wider self-theme that makes you vulnerable to create doubt in specific domains."
- This self-theme also provides more insight regarding type of OCD, trigger situations as well as roadblocks to change.
- During IBT, the vulnerable self theme is deconstructed and challenged. The re-authoring of this self-theme is an integral part of the goals of reality sensing and behavioral change.
- There is a dynamic inter-play between thematic shifts in narratives of vulnerability and the trust required in behavior change
- Through constant repetition of this type of "grounded doing" and sensing reality, there is a consolidation of self and the rediscovered relationship with the world as it really is.
- This change is quite transformative such that oftentimes new life possibilities and goals emerge.
For a more detailed summary of the stages and steps in IBT, click on the button below
References
American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, (Copyright 2013).
Aardema, F., Radomsky, A.S., O'Connor, K.P., Julien, D. (2009). Inferential Confusion, Obsessive Beliefs and Obsessive-Compulsive Symptoms: A Multidimensional Investigation of Cognitive Domains. Clinical Psychology and Psychotherapy, 15(4), 227-238
Aardema, F., O'Connor, K. P., & Emmelkamp, P. M. G. (2006). Inferential Confusion and Obsessive Beliefs in Obsessive‐Compulsive Disorder. Cognitive Behaviour Therapy, 35(3), 138–147.
Beckman. J., Bloch. M., King. R., (2009) Symptom Dimensions and Subtypes of Obsessive Compulsive Disorder: A Developmental Perspective. Dialogues In Clinical Neuroscience, Vol 11 (1)
Foa, Edna., (2010) Cognitive Behavioral Therapy of Obsessive-Compulsive Disorder Dialogues Clinical Neuroscience, 12(2): 199–207
McKay. D., Abramowitz. J., Calamari.. J., Kyrois. M., Radomsky. A., Sookman. D., Taylor. S., Wilhelm, S., (2004) A critical evaluation of obsessive–compulsive disorder subtypes: Symptoms versus mechanisms. Clinical Psychology Review 24: 283–313
O’Connor. K., Ecker, Lahoud, M., Roberts. S., A Review of the Inference-Based Approach to Obsessive Compulsive Disorder. Verhaltenstherapie (2012); 22:47–55
O'Connor, K., Koszegi, N., Aardema, F., van Niekerk, J., & Taillon, A. (2009). An inference-based approach to treating obsessive-compulsive disorders. Cognitive and Behavioral Practice, 14(4), 420-429.
Pélissier, M.-C., & O'Connor, K. P. (2002). Deductive and inductive reasoning in obsessive-compulsive disorder. British Journal of Clinical Psychology, 41(1), 15–27. https://doi.org/10.1348/014466502163769
Taylor. S., Dimensional and Subtype Models Of OCD. Abramowitz. J., (2005) Concepts and Controversies in Obsessive-Compulsive Disorder. Hosts, A.C. (Eds). XVIII, 438 P
Whittal, Maureen L., Thordarson, Dana S., McLean, Peter D. (2005). Treatment of obsessive–compulsive disorder: Cognitive behavior therapy vs. exposure and response prevention. Behaviour Research and Therapy, 43(12) 1559–1576
Wilhelm, S., & Steketee, G. (2006). Treating OCD with Cognitive Therapy. Oakland, CA: New Harbinger.

Treatment of Obsessional Spectrum Anxiety
6 Harris Street, Newburyport, MA 01950